
This website is best viewed using the vertical display on your mobile device.
This site is intended for US-based Healthcare Professionals only.
- SPRYCEL Patient Site
- BMS Resources
- Full Prescribing Information
- Indications

INDICATIONS
SPRYCEL® (dasatinib) is indicated for the treatment of adult patients with:
- Newly diagnosed Philadelphia chromosome-positive (Ph+) chronic myeloid leukemia (CML) in chronic phase
- Chronic, accelerated, or myeloid or lymphoid blast phase Ph+ CML with resistance or intolerance to prior therapy including imatinib
- Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ ALL) with resistance or intolerance to prior therapy
SPRYCEL® is indicated for the treatment of pediatric patients 1 year of age and older with:
- Newly diagnosed Philadelphia chromosome-positive (Ph+) acute lymphoblastic leukemia (ALL) in combination with chemotherapy
- Philadelphia chromosome-positive (Ph+) chronic myeloid leukemia (CML) in chronic phase

SPRYCEL patients achieved higher & faster cCCyR* and MMR† rates at Years 1 and 5 vs imatinib1‡
DASISION Trial design
- Results based on a Phase III, open-label, randomized study of SPRYCEL® (dasatinib) 100 mg (n=259) once daily vs imatinib 400 mg once daily (n=260) in adults with newly diagnosed CP Ph+ CML (N=519)1,2
- Primary endpoint was the rate of cCCyR by 12 months1,2
- Select secondary endpoints included: MMR at any time, time to MMR, and time to cCCyR1,2
- cCCyR* RatesYear 1 & 5 Data
- MMR† RatesYear 1 & 5 Data
- Transformation Rates

More patients achieved cCCyR at Year 1 and Year 5
vs imatinib1

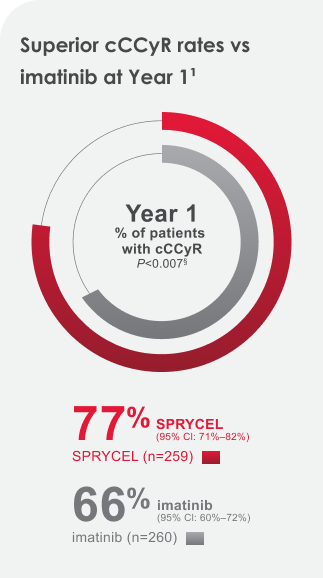


77% of SPRYCEL patients achieved the cCCyR 12-month treatment milestone. 83% achieved the Year 5 treatment milestone.1
IMPORTANT INFORMATION ABOUT ADVERSE REACTIONS
In newly diagnosed chronic phase CML patients:
- Drug-related serious adverse reactions (SARs) were reported for 16.7% of SPRYCEL-treated patients. Serious adverse reactions reported in ≥5% of patients included pleural effusion (5%)
- The most common adverse reactions (≥15%) include myelosuppression, fluid retention, and diarrhea
SPRYCEL helped patients achieve cCCyR faster at a median time to response of 3.1 months
after 5-year follow-up1,2


More patients achieved higher and faster MMR rates Year 1 through Year 5 on SPRYCEL
vs imatinib1,4
Achieving MMR is important on a patient’s treatment path5




Cumulative rates of MMR and
molecular responses with a 4.0- or 4.5-log reduction in BCR-ABL1 transcripts
from baseline by 5 years remained statistically significantly higher for
dasatinib vs imatinib.7
IMPORTANT INFORMATION ABOUT ADVERSE REACTIONS
- With a minimum of 60 months follow-up, adverse reactions that were reported in
≥10% of patients with newly diagnosed chronic phase CML for patients taking
SPRYCEL (n=258) included:
- All grades: fluid retention (38%) [including pleural effusion (28%), superficial localized edema (14%), pulmonary hypertension (5%), generalized edema (4%), pericardial effusion (4%), congestive heart failure/cardiac dysfunction|| (2%), pulmonary edema (1%)], diarrhea (22%), musculoskeletal pain (14%), rash¶ (14%), headache (14%), abdominal pain (11%), fatigue (11%), nausea (10%), myalgia (7%), arthralgia (7%), hemorrhage# (8%) [including gastrointestinal bleeding (2%), other bleeding** (6%)], vomiting (5%), muscle spasms (5%)
- Grade 3/4: fluid retention (5%) [including pleural effusion (3%), pulmonary hypertension (1%), pericardial effusion (1%)], diarrhea (1%), hemorrhage (1%) [including gastrointestinal bleeding (1%)]
On SPRYCEL, more patients achieved MMR Year 1 through Year 5
vs imatinib1,8


After 5 years of follow-up, median time to MMR among responders was 9.3 months in the SPRYCEL arm (n=198) and 15 months in the imatinib arm (n=167)1
5-year MMR rates across all Hasford risk scores with
SPRYCEL1


Baseline Hasford risk scores1,2
- SPRYCEL: low: 33% (n=86);
intermediate: 48% (n=124);
high: 19% (n=49) - imatinib: low: 34% (n=87);
intermediate: 47% (n=123); high: 19% (n=50)
97% of patients on SPRYCEL remained in the chronic phase over a minimum of 5
years’ follow-up1
Patient transformations by year while on study9


SPRYCEL patients experienced no new transformations after Year 3 and continuing through Year 59


Imatinib patients experienced 2 new transformations after Year 3 and continuing through Year 59
94% of imatinib-treated patients on study did not transform to accelerated phase or blast crisis (245/260)1,9
All randomized patients who transformed while on study progressed to either accelerated phase or blast crisis.1
- Lack of transformation to accelerated or blast phase is a key indicator of lack of disease progression10
IMPORTANT INFORMATION ABOUT MYELOSUPPRESSION
Treatment with SPRYCEL is associated with severe (NCI CTCAE Grade 3/4) thrombocytopenia, neutropenia, and anemia, which occur earlier and more frequently in patients with advanced phase CML or Ph+ ALL than in patients with chronic phase CML. Myelosuppression was reported in patients with normal baseline laboratory values as well as in patients with pre-existing laboratory abnormalities.
- In patients with chronic phase CML, perform complete blood counts (CBCs) every 2 weeks for 12 weeks, then every 3 months thereafter, or as clinically indicated
- Myelosuppression is generally reversible and usually managed by withholding
SPRYCEL temporarily and/or dose reduction
- In clinical studies, myelosuppression may have also been managed by discontinuation of study therapy
- Hematopoietic growth factor has been used in patients with resistant myelosuppression
Dasatinib does not appear to be active against the T315I mutation, based on in vitro data.1
BCR-ABL=breakpoint cluster region-Abelson kinase; cCCyR=confirmed complete cytogenetic response; CI=confidence interval; CP=chronic phase; MMR=major molecular response; Ph+ CML=Philadelphia chromosome-positive chronic myeloid leukemia; RQ-PCR=real-time quantitative polymerase chain reaction.
*cCCyR was defined as CCyR (0% Ph+ metaphases) on 2 consecutive occasions at least 28 days apart.1,2
†MMR (at any time) defined as BCR-ABL ratios of ≤0.1% by RQ-PCR in peripheral blood samples standardized on the International Scale. These are cumulative rates representing minimum follow-up for the time frame specified.1,2
‡Inclusive of cCCyR in newly diagnosed adult patients with CP Ph+ CML by 1 and 5 years.1
§Adjusted for Hasford score and indicated statistical significance at a predefined nominal level of significance.1
||Includes cardiac failure acute, cardiac failure congestive, cardiomyopathy, diastolic dysfunction, ejection fraction decreased, and left ventricular dysfunction.1
¶Includes erythema, erythema multiforme, rash, rash generalized, rash macular, rash papular, rash pustular, skin exfoliation, and rash vesicular.1
#Adverse reaction of special interest with <10% frequency.1
**Includes conjunctival hemorrhage, ear hemorrhage, ecchymosis, epistaxis, eye hemorrhage, gingival bleeding, hematoma, hematuria, hemoptysis, intra-abdominal hematoma, petechiae, scleral hemorrhage, uterine hemorrhage, and vaginal hemorrhage.1
See efficacy results for adults with Ph+ CML in CP
resistant or intolerant to imatinib
resistant or intolerant to imatinib
References:
- SPRYCEL full Prescribing Information. Bristol-Myers Squibb Company.
- Kantarjian H, Shah NP, Hochhaus A, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2010;362(24):2260-2270.
- Baccarani M, Saglio G, Goldman J, et al. Evolving concepts in the management of chronic myeloid leukemia: recommendations from an expert panel on behalf of the European LeukemiaNet. Blood. 2006;108:1809-1820.
- Kantarjian H, Shah NP, Cortes JE, et al. Dasatinib or imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: 2-year follow-up from a randomized phase 3 trial (DASISION). Blood. 2012;119(5):1123-1129.
- Cortes J, Quintas-Cardama A, Kantarjian HM. Monitoring molecular response in chronic myeloid leukemia. Cancer. 2011;117(6):1113-1122.
- Jabbour E, Kantarjian H, Saglio G, et al. Early response with dasatinib or imatinib in chronic myeloid leukemia: 3-year follow-up from a randomized phase 3 trial (DASISION). Blood. 2014;123(4):494-500.
- Cortes JE, Saglio G, Kantarjian HM, et al. Final 5-year study results of DASISION: the dasatinib versus imatinib study in treatment-naïve chronic myeloid leukemia patients trial. J Clin Oncol. 2016;34(20):2333-2340.
- Data on file. SPRY 064. Bristol-Myers Squibb Company; 2016.
- Data on file. SPRY 061. Bristol-Myers Squibb Company; 2016.
- Bavaro L, Martelli M, Cavo M, Soverini S. Mechanism of disease progression and resistance to tyrosine kinase inhibitor therapy in chronic myeloid leukemia: an update. Int J Mol Sci. 2019;20(24):6141.
DASISION Trial: SPRYCEL vs imatinib study in treatment-naïve CP Ph+ CML adult patients1,2
Phase III, open-label, international, multicenter, randomized study1,2


*Patient characteristics were well balanced between treatment arms, including age, gender, disease
characteristics, and Hasford risk stratification.
Primary endpoint:
cCCyR† by 12 months1,2
cCCyR† by 12 months1,2
Select secondary endpoints included:
MMR‡ at any time, time to MMR, and time to cCCyR2
MMR‡ at any time, time to MMR, and time to cCCyR2
- Patients with a history of cardiac disease were included in this study, except those who had an MI within 6 months, congestive heart failure within 3 months, significant arrhythmias, or QTc prolongation1
- Patients continued to receive the study treatment until the disease progressed or unacceptable toxic effects developed. Interruptions of therapy or dose reductions or escalations were allowed in the case of both treatments2
- With a minimum of 5 years of follow-up, 61% of SPRYCEL® (dasatinib) patients and 62% of imatinib patients were still on study1
- At baseline, Hasford risk scores for the SPRYCEL and imatinib treatment groups, respectively1:
- Low risk: 33% and 34%
- Intermediate risk: 48% and 47%
- High risk: 19% and 19%
Key inclusion criteria2
- Diagnosis of chronic phase Philadelphia chromosome-positive CML within 3 months before study entry
- No prior treatment for CML except for hydroxyurea or anagrelide
- ECOG performance 0-2
- Adequate organ function, including hepatic and renal function
- Aged 18 years or older
Key exclusion criteria2
- Serious uncontrolled medical disorders or active infections
- History of serious bleeding disorder unrelated to CML
- Pleural effusion at baseline
- Previous or concurrent cancer (other than basal-cell skin cancer)
cCCyR=confirmed complete cytogenetic response; MMR=major molecular response.
†cCCyR was defined as CCyR (0% Ph+ metaphases) on 2 consecutive occasions at least 28 days apart.1,2
‡MMR (at any time) was defined as BCR-ABL ratios ≤0.1% by RQ-PCR in peripheral blood samples standardized on the International Scale. These are cumulative rates representing minimum follow-up for the time frame specified.1
SPRYCEL can cause serious and fatal bleeding. In all CML or Ph+ ALL clinical studies, Grade ≥3 central nervous system (CNS) hemorrhages, including fatalities, occurred in <1% of patients receiving SPRYCEL. The incidence of Grade 3/4 hemorrhage occurred in 5.8% of patients and generally required treatment interruptions and transfusions. The incidence of Grade 5 hemorrhage occurred in 0.4% of patients. The most frequent site of hemorrhage was gastrointestinal.
- Most bleeding events in clinical studies were associated with severe thrombocytopenia
- In addition to causing thrombocytopenia in human subjects, dasatinib caused platelet dysfunction in vitro
- Concomitant medications that inhibit platelet function or anticoagulants may increase the risk of hemorrhage
References:
- SPRYCEL full Prescribing Information. Bristol-Myers Squibb Company.
- Kantarjian H, Shah NP, Hochhaus A, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2010;362(24):2260-2270.